Why consider TaTME?
Colin Sietses
The Challenge of Deep Pelvic Dissection
Using a trans-abdominal approach, dissection of the deep pelvis is challenging. The funnel-shape of the pelvis plays an important role in the complexity of rectal cancer surgery. It limits working space and dissection becomes more difficult the deeper one goes. Factors that limit the surgeon’s working space include the solid nature and limited internal dimensions of the bony pelvis, the size of the prostate, and the muscularity of the pelvic floor. In some patients, a bulky mesorectum also contributes to the difficulty of a trans-abdominal dissection in the deep pelvis.
This difficult dissection poses several risks to the patient.
These include:
- Inadvertent injury to hypogastric nerves with resultant sexual and urinary dysfunction
- Substantial manipulation of the mesorectal specimen with disruption of its enveloping fascia and comrpomise of surgical margins
- Unplanned dissection in the prostate or vaginal wall due to poor visibility during the anterior portion of deep pelvic dissection
- Inadequate distal margin due to difficulty of transabdominal dissection in or near the pelvic floor
- Intraluminal tumor contamination of the distal anorectal canal during manipulation
- Imperfect stapling of the distal margin due to the steep angulation of the deep pelvis
Potential benefits of TaTME technique:
To our opinion there are several potential benefits of approaching the rectum from below and performing a transanal mesorectal dissection.
Improvements in Deep Pelvic Dissection Noted with TaTME
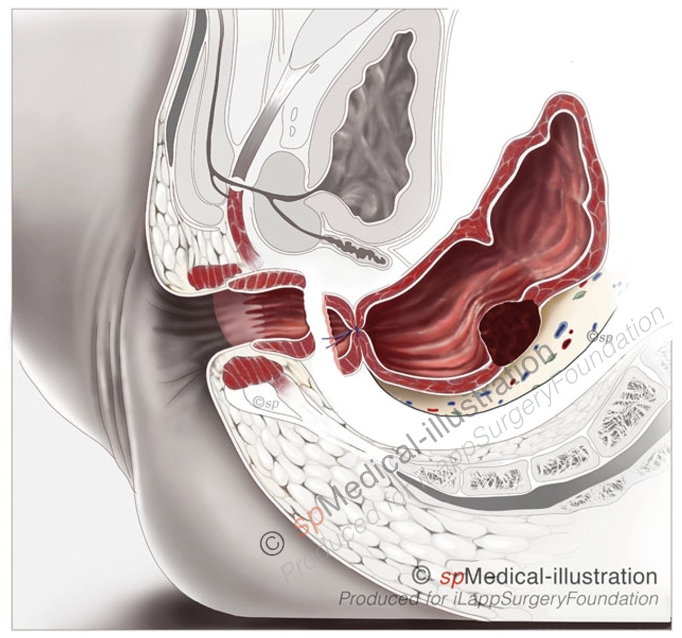
1. Better visualization of nerve bundles
Injury to the hypogastric nerve branches in the deep pelvis is avoided by excellent visualization of the pelvic floor muscle layers and mesorectal space posteriorly, prior to dissection of the lateral attachments.
2. Reduced specimen manipulation
The use of the pneumorectum to aid in dissection, and with improved visualization of the deep pelvic structure, less manipulation of the mesorectum and specimen margins is required by a TaTME approach.
3. Anterior dissection in male patients
With a TaTME approach, the anterior dissection is more exact with excellent visualization of the prostate and rectovaginal septum, and offers the ability to decide whether to stay in front or behind Denonviller’s fascia.
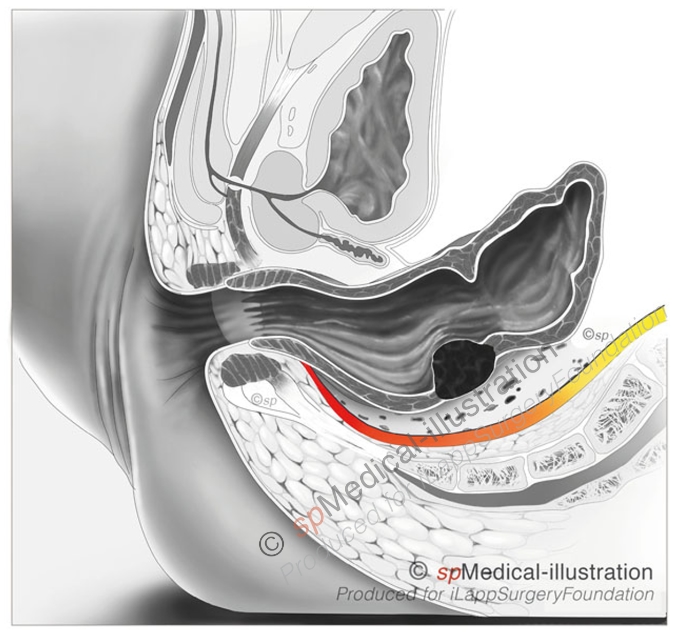
4. Improved visualization of distal margin
With a transanal approach, the distal edge of tumor can be directly visualized and the distal margin chosen before starting dissection. A transanal endoscopic approach also allows a very low dissection under direct vision.
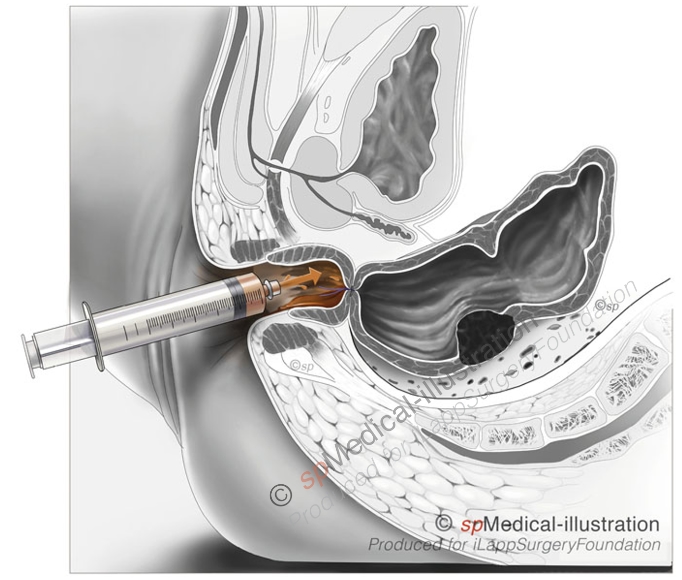
5. Possibility for improved washout
After performing a trans-anal gas-tight pursestring suture below the tumor, complete washout of the residal anorectal space is possible and to our opinion even necessary. This could improve oncologic results.
6. Avoiding imperfect distal stapling
Currents staplers are limited in their angulation and perpendicular distal stapling of the rectum is difficult – whether performed open or laparoscopically. Incomplete TME-specimens can result from coning into the specimen on the distal margin. With the TaTME-technique a perfect rectotomy can be performed and distal stapling is avoided.

Although we focus on rectal cancer treatment there are other indications for TaTME, like IBD, restorage of continuity and treatment of fistulae.
Because TaTME is a new and difficult technique, we advocate the implementation of it in a stepwise way and through a CV containing dry and wetlab and well organized proctoring.